Kora Behavioral Health alcohol detox is often imagined in extremes—cold sweats, shaking, or someone strapped to a hospital bed. That image isn’t entirely fictional, but it also doesn’t reflect the full reality of modern detox care.
In practice, alcohol detox is a medically supervised process designed to keep patients safe, monitored, and supported while withdrawal symptoms are managed. The fear of severe withdrawal is real, but structured treatment exists specifically to reduce risk and make the process as safe as possible under clinical supervision.
What happens during alcohol detox is a medically supervised process that helps the body safely clear alcohol while managing withdrawal symptoms. When someone stops drinking after regular or heavy use, the nervous system can react with symptoms like anxiety, tremors, nausea, and insomnia within the first 6–24 hours.
In a supervised setting, medical staff monitor symptoms, provide medications when needed, and support stabilization as the body adjusts. Detox usually lasts several days before transitioning into ongoing treatment or recovery care.
This walkthrough covers the real sequence of events, from the first admissions call through discharge planning, so you know what’s coming at every step.
What you’ll learn:
- What the intake and medical assessment actually involves
- How your individualized care plan gets built
- What the withdrawal timeline typically looks like
- Which medications are used and why
- What happens after detox ends
The Intake and Medical Assessment
The first few hours aren’t dramatic. Mostly, they involve paperwork, conversation, and a physical exam. The clinical team needs to understand who you are before they can figure out how to take care of you safely, and that process begins the moment you arrive.
You’ll go through a medical history review, a structured alcohol use assessment, and a physical examination. Vital signs get collected. A mental health screening happens, too, because alcohol use disorder and co-occurring conditions like anxiety or depression are deeply entangled for a lot of people. Any medications you’re currently taking get reviewed, both for safety and because some substances can complicate the withdrawal picture in ways that aren’t immediately obvious.
What the clinical team is really building during intake is a withdrawal risk profile. According to SAMHSA’s clinical guidelines, structured assessment tools like the CIWA-Ar scale are used to evaluate withdrawal severity systematically, which allows the team to calibrate monitoring intensity and medication strategy before symptoms escalate.
What Information You’ll Be Asked For
The intake conversation covers a lot of ground, and it’s worth knowing this ahead of time so nothing catches you off guard:
- How long you’ve been drinking heavily and approximately how much
- Whether you’ve attempted detox or abstinence before
- Any prior withdrawal symptoms, including seizures or hallucinations
- Existing medical conditions and current prescriptions
- Mental health history and any active diagnoses
None of this is interrogation. The team is building a safety map. Prior withdrawal experiences matter a great deal clinically, because the nervous system can “remember” previous withdrawal episodes in a way that makes subsequent ones more intense, a phenomenon sometimes called the kindling effect.
Building Your Individualized Detox Plan

After the intake assessment wraps up, the clinical team puts together a care plan specific to you. Not a template. Not a standard protocol handed to everyone who walks through the door.
Age, overall health status, duration and severity of heavy drinking, liver function, and any co-occurring mental health disorders all shape what the plan looks like. Someone who has been drinking heavily for two decades with a history of delirium tremens needs a fundamentally different level of care than someone experiencing their first significant withdrawal. The ASAM Alcohol Withdrawal Management Guidelines make this individualization explicit, establishing patient placement criteria based on medical complexity rather than a one-size approach.
Why No Two Detox Experiences Are Identical
This is the part that surprises people. The word “detox” sounds like a fixed experience, but it’s really a category of care. Two people walking into the same facility on the same day can have completely different monitoring schedules, medication regimens, and clinical interactions based on their individual risk factors.
Mental health factors carry particular weight here. A person managing severe anxiety or a mood disorder alongside alcohol withdrawal symptoms faces a layered clinical picture that requires careful coordination between physical stabilization and psychiatric support.
24/7 Monitoring Explained
Continuous monitoring during alcohol withdrawal isn’t precautionary theatre. It exists because withdrawal from alcohol is one of the few substance withdrawal syndromes that can actually kill you, and the danger doesn’t always announce itself loudly.
Vital signs get checked regularly throughout the day and night. Withdrawal symptom severity gets tracked on a structured scale, allowing the clinical team to spot deterioration early and adjust treatment before things escalate. The monitoring is quiet, mostly. Check-ins, conversations, assessments. It doesn’t feel like surveillance so much as consistent attention.
Why Monitoring Matters During Alcohol Withdrawal
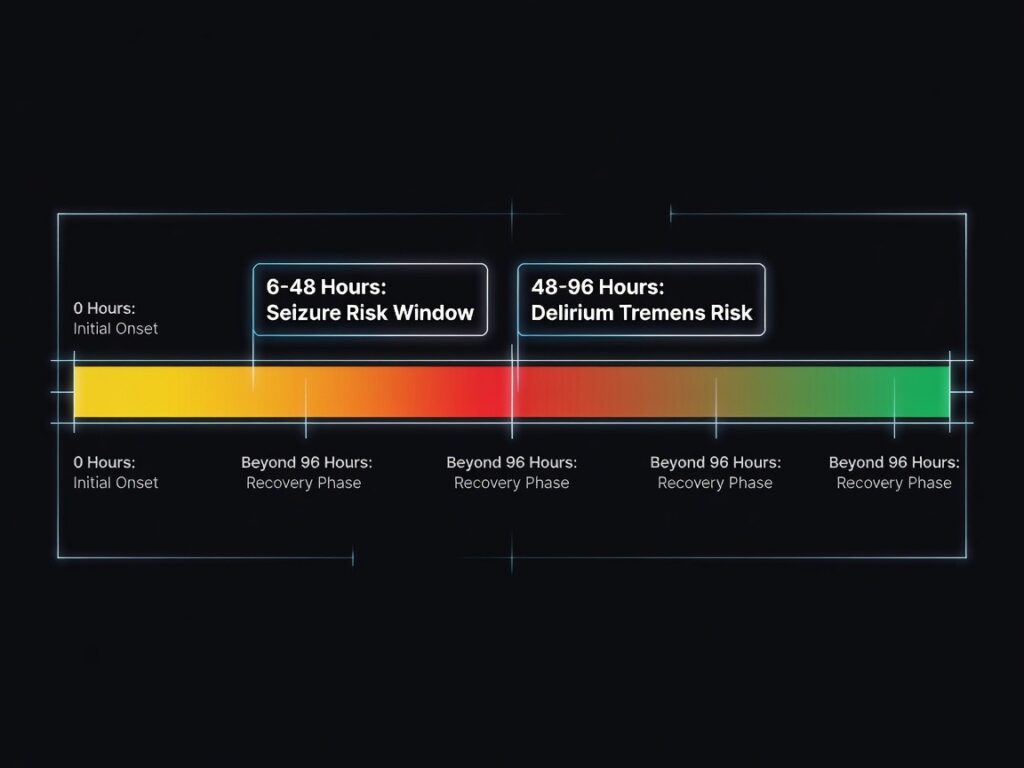
The specific risks that monitoring is designed to catch are serious. Seizures can emerge anywhere between 6 and 48 hours after the last drink, often without any preceding warning signs. Delirium tremens, the most dangerous stage of severe alcohol withdrawal, typically develops between 48 and 96 hours after cessation and carries a mortality risk that is significantly higher in unsupervised settings. Blood pressure can spike unexpectedly. Severe dehydration can develop quickly. The clinical team isn’t hovering out of habit; they’re watching for a narrow window of time when the body’s CNS recalibration can go sideways in ways that require immediate intervention.
Medications You May Receive
This is the section that tends to generate the most anxiety, and I suspect it’s because people picture being sedated into submission or handed something that creates a new dependency. The reality is far more measured.
Alcohol detox process step by step involves individualized medical care, and medication decisions are based on a withdrawal risk assessment completed at intake. Not everyone receives the same treatment protocol. Some individuals require more intensive pharmacological support to manage withdrawal symptoms safely, while others may need only minimal intervention depending on severity and medical history.
Throughout detox, clinical staff monitor symptoms closely and adjust medications as needed to ensure safety, comfort, and stabilization during the withdrawal process.
The goal across the board is the same: reduce withdrawal severity, improve safety, and support physical stabilization.
The clinical evidence base for managing alcohol withdrawal is well-established. Benzodiazepines are the most extensively studied class for managing acute withdrawal symptoms, particularly for seizure prevention. Other medication categories address specific symptom clusters, nausea, insomnia, elevated blood pressure, and nutritional deficiencies that are extremely common in people with heavy alcohol use histories, especially thiamine depletion, which carries its own serious neurological risks if left unaddressed.
What Medications Are Designed to Do
What to expect in alcohol detox is a medically structured process where the goal is safety, not comfort alone. Withdrawal medications are not given to make detox “easy,” but to reduce the risk of serious or life-threatening complications that can occur when alcohol dependence is stopped abruptly.
In many cases, care also includes nutritional support and IV hydration. Long-term alcohol use can leave the body depleted of fluids, electrolytes, and essential vitamins, which can worsen withdrawal symptoms if not addressed. Replenishing these is a standard part of treatment, alongside medical monitoring and symptom management, to help stabilize the body during the detox process.
Managing Symptoms Day by Day
Here’s where the actual lived experience of detox lives. The timeline varies meaningfully from person to person, and anyone who gives you a rigid hour-by-hour script is probably oversimplifying. That said, the general shape of the withdrawal progression follows a recognizable pattern.
| Timeframe | Typical Symptom Pattern |
| First 6–24 hours | Anxiety, tremors, insomnia, nausea, elevated heart rate, sweating |
| Days 2–3 | Peak symptom intensity for most people; seizure and DTs risk window is active |
| Days 4–5 | Symptoms begin stabilizing for many patients; sleep remains disrupted |
| Days 6–7+ | Ongoing fatigue, mood changes, appetite changes; acute phase resolving |
Appetite tends to be poor throughout, and sleep quality is often rough even after the acute symptoms settle. Anxiety and restlessness can linger well past the physical peak. That post-acute phase isn’t weakness; it’s the CNS continuing to find its equilibrium after prolonged suppression by ethanol. The Cleveland Clinic’s clinical overview describes this progression as spanning roughly three to eight days for the acute phase, though longer-term psychological symptoms can persist beyond that window.
Therapy That Starts During Detox

Physical stabilization is the urgent priority, but it doesn’t occupy every hour of every day. Most medically supervised programs introduce counseling and therapeutic support early, during active detox, rather than waiting until the body is fully stabilized.
That early clinical contact matters more than it might seem on the surface. Motivation and ambivalence about recovery shift constantly, and catching someone during a window of genuine openness, which the detox period often represents, can anchor commitment in ways that purely physical treatment can’t.
You might meet with a counselor individually, attend a brief group session, or work through recovery education material. Mental health screening continues throughout, with particular attention to mood changes and psychiatric symptoms that can emerge as withdrawal progresses. For patients whose families are involved in their care, communication with loved ones, with appropriate consent, often begins during this phase as well.
Transitioning to Ongoing Treatment
This is the part that tends to get glossed over, and it probably shouldn’t. Detox stabilizes your body. It does not treat alcohol use disorder. Those are related but genuinely distinct objectives, and conflating them is one of the more consequential misunderstandings in how people think about recovery.
Research from the NIAAA consistently demonstrates that detox followed by no continuing care produces significantly higher relapse rates than detox integrated into a broader treatment continuum. The neurological and psychological factors driving alcohol addiction treatment needs don’t resolve during a five-to-seven-day detox stay.
Why Detox Alone Is Rarely Enough
Alcohol use disorder has roots that physical withdrawal doesn’t touch. The underlying patterns, trauma, mental health conditions, behavioral habits, environmental triggers, are still fully intact when someone walks out of detox. Ongoing treatment, whether that’s residential rehabilitation, intensive outpatient programming, or dual-diagnosis-focused therapy, addresses those roots. Detox is the necessary first step. It clears the physiological ground for actual recovery work to begin.
What Discharge Looks Like
Discharge isn’t abrupt. Before anyone leaves, the clinical team conducts a review of where the patient is medically and where they’re going next. Transition recommendations get made based on the individualized assessment, not a default prescription.
If medications are being continued beyond the detox stay, instructions are clear and specific. Follow-up appointments get scheduled or coordinated. Referrals to the next level of care, whether inpatient rehab, outpatient treatment, or community recovery support, are built into the discharge plan rather than left to the patient to figure out independently afterward.
The honest thing to say about discharge is that leaving detox without a concrete continuing care plan dramatically increases vulnerability. The first weeks after acute withdrawal resolve are statistically among the highest-risk periods for relapse, and discharge planning exists precisely to bridge that gap.
Ready to Learn What Detox Could Look Like for You?
Kora Behavioral Health alcohol detox is never a one-size-fits-all experience. Every person’s detox process is shaped by their own history, overall health, and specific withdrawal risk profile. Because of that, outcomes and care plans can vary significantly from one individual to another.
In practice, speaking with a clinical team before committing to treatment can help clarify what to expect in your specific situation. Instead of relying on general information, you can get guidance tailored to your symptoms, medical background, and level of alcohol use, which makes the next steps clearer and more informed.
If you’re in central Pennsylvania, including Lancaster, York, Harrisburg, Hershey, Reading, or Lebanon, Kora Behavioral Health offers confidential detox consultations with no obligation attached. You can reach them directly at (866) 861-9667, or explore alcohol detox options to get a clearer sense of what care could look like for you.
FAQs
What is the first day of detox like?
The first day is primarily intake and assessment. You’ll go through a medical history review, a physical examination, mental health screening, and a structured alcohol use assessment. Vital signs get taken and monitored. The clinical team builds your withdrawal risk profile and begins establishing your individualized care plan. Most people find the first day more administrative than dramatic, though withdrawal symptoms may already be present depending on when the last drink occurred.
Will I be in pain during detox?
Symptoms vary widely and depend heavily on how long and how heavily someone has been drinking. Medical teams work to manage discomfort throughout, and the continuous monitoring that occurs during detox allows clinicians to respond quickly when symptoms become distressing. The goal is safety and stabilization, which includes keeping unnecessary suffering to a minimum through appropriate clinical intervention.
What happens after detox ends?
Discharge from detox comes with a transition plan. Most clinical teams recommend continuing into a higher level of care, such as residential rehabilitation or intensive outpatient treatment, because the underlying factors driving alcohol use disorder aren’t resolved by physical stabilization alone. Recovery planning, therapy referrals, and follow-up coordination are standard components of the discharge process, designed to support the longer-term work that detox makes possible.

