
Kora Behavioral Health alcohol detox often begins with uncertainty. When someone decides they need help with alcohol, the first questions are rarely about whether to get better—they’re more practical: can I keep working, do I need inpatient care, or is outpatient detox safe for me?
These questions matter because the answer isn’t the same for everyone. Alcohol withdrawal can range from mild to medically serious, and choosing the wrong level of care isn’t just inconvenient—it can be dangerous. That’s why the first step is usually a clinical assessment to determine the safest and most appropriate setting for detox.
Both inpatient and outpatient alcohol detox work. Neither is universally superior. What separates them isn’t the quality of care so much as the intensity of monitoring, the structure of daily life during detox, and how much medical intervention is available if something goes south. The ASAM Criteria, which clinicians use as the standard framework for matching patients to appropriate levels of care, makes this distinction clearly: placement should reflect clinical need, not scheduling convenience.
This guide breaks down what actually differs between these two settings, who belongs in each one, and how the decision gets made when a real clinician is in the room.
The Two Main Detox Settings
Inpatient vs outpatient alcohol detox comes down to the level of medical support, supervision, and structure needed during withdrawal.
Inpatient detox means you’re admitted to a facility and stay there full-time, typically for three to seven days or longer, depending on clinical need. You sleep, eat, and receive care on-site with 24/7 monitoring by medical staff. Medications such as benzodiazepines or phenobarbital can be administered immediately if withdrawal symptoms escalate, which allows for rapid response without delays in care.
This level of treatment removes barriers like transportation or waiting between symptom onset and medical support, making it the safest option for people at higher risk of severe withdrawal.
Outpatient detox looks completely different in practice. You show up to a clinic or treatment center — maybe once a day, maybe several times a week — receive your medication and clinical assessment, then go home. You’re still under medical supervision, but it’s scheduled and structured rather than continuous. The assumption is that between appointments, your symptoms remain stable and your home environment is safe.
What they share is more important than people realize. Both involve clinical evaluation before anything starts, both use evidence-based protocols to manage alcohol withdrawal symptoms, and both are designed as a bridge into longer-term treatment — not an endpoint in themselves. Detox, inpatient or outpatient, stabilizes the body. Recovery happens afterward.
| Feature | Inpatient Detox | Outpatient Detox |
| Monitoring | 24/7 on-site | Scheduled daily or multi-weekly visits |
| Living Arrangement | Residential, facility-based | Patient remains at home |
| Emergency Response | Immediate | Escalation protocol required |
| Typical Duration | 3–10 days | 5–14 days depending on protocol |
| Best For | Severe dependence, high medical risk | Mild-to-moderate risk, stable home |
| Cost Range | Higher | Significantly lower |
Similarities Between Both Options
Both settings begin with a thorough medical intake. Both use validated withdrawal assessment tools like the CIWA-Ar scale to track symptom severity. Both programs are supposed to connect patients to the next phase of treatment — whether that’s residential rehab, an intensive outpatient program, or ongoing counseling. The goal in either case is medical stabilization, not a cure. Anyone who tells you detox alone is sufficient treatment for alcohol use disorder is glossing over what the research actually says.
Who Needs Inpatient Detox?
Alcohol withdrawal is one of the few substance withdrawals that can kill you. That’s not dramatic language — it’s a clinical reality. Delirium tremens, which occurs in roughly 3–5% of people going through withdrawal, carries a mortality rate of up to 15% when untreated. Seizures can occur within six to 48 hours of the last drink, sometimes without any warning at all.
So who genuinely needs inpatient care? People with a history of complicated withdrawal — prior seizures, prior episodes of delirium tremens, or prior hospitalizations during detox — are at substantially higher risk the next time. That history matters more than how much someone is currently drinking. People who have been drinking heavily for years, particularly those consuming more than ten standard drinks a day, are also flagged as high-risk because the physiological dependence tends to be deeper.
Co-occurring medical conditions change the calculus too. Liver disease, cardiovascular problems, severe anxiety or panic disorders, and certain psychiatric conditions all increase the complexity of managing withdrawal safely. Pregnancy falls into its own category entirely and almost always warrants medical inpatient monitoring given the stakes involved for two people.
Then there’s the environmental question. Someone whose home is where they drink, where their using friends stop by, where the stress that drives the drinking lives — that person is trying to withdraw in the same conditions that created the problem. Even if the medical risk were low, the relapse risk inside that environment is high.
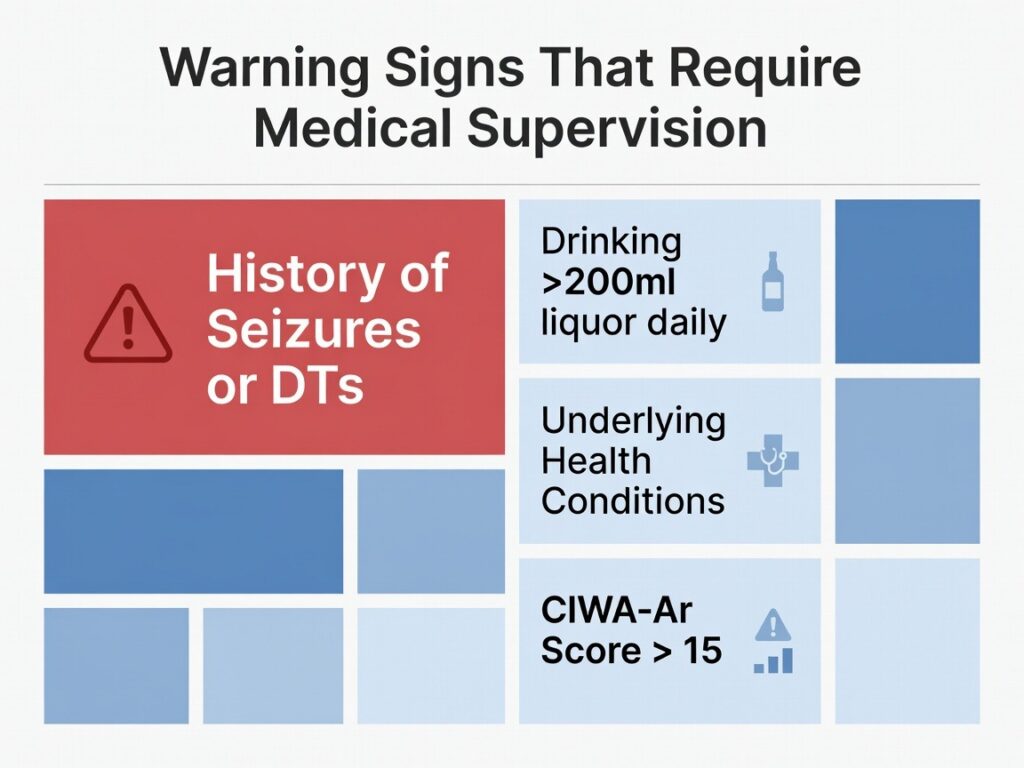
Warning Signs That Require Medical Supervision
- History of alcohol-related seizures or delirium tremens during a previous withdrawal
- Drinking more than half a fifth of liquor (roughly 200ml or more) daily for an extended period
- Significant underlying health conditions, including heart disease or severe liver dysfunction
- Clinical assessment findings indicating a CIWA-Ar score above 15, which signals moderate-to-severe withdrawal risk
When Outpatient Detox Is Appropriate
Outpatient detox gets undersold and misunderstood simultaneously. It’s not a consolation prize. For the right person, it’s genuinely the smarter option — less disruptive, less expensive, and when matched correctly to clinical risk, research published in peer-reviewed literature shows outcomes comparable to inpatient care.
The operative phrase there is “matched correctly.” Outpatient is appropriate when the withdrawal risk is mild to moderate — meaning someone who hasn’t had prior complicated withdrawals, who isn’t drinking at catastrophic daily volumes, and who doesn’t have serious complicating medical conditions. A clinician will typically look at CIWA-Ar scores at intake: below a certain threshold, outpatient management is defensible and often preferred.
What matters just as much as medical risk is the logistical reality of the patient’s life. Reliable transportation to daily or near-daily appointments is non-negotiable. A stable living situation — ideally with a sober or supportive person at home — is critical. The ability to actually show up, every scheduled visit, without skipping because work got complicated or motivation dipped, is what separates outpatient success from outpatient failure.
Frankly, I suspect most people who underestimate outpatient are thinking of it as “doing it alone.” It’s not. There’s physician oversight, medication management, and a clinical escalation plan if things worsen. The structure is different from inpatient, but it’s still medical care.
When Outpatient Detox May Not Be Recommended
The list of situations where outpatient becomes risky is worth understanding clearly. High-risk withdrawal history disqualifies most people immediately. Unstable living situations — including active domestic conflict, housing insecurity, or a home where alcohol is present — create conditions where even a well-run outpatient program can’t compensate for what happens between appointments. Significant medical complications, or simply being unable to attend scheduled monitoring visits reliably, both tip the clinical scale toward inpatient.
Safety Differences That Matter
The core safety distinction between these two settings comes down to what happens in hour two, or hour nine, or at 3 a.m. when something changes. Inpatient facilities have nursing staff present continuously. Labs can be drawn immediately. Medications can be escalated the moment a patient’s CIWA-Ar score climbs. The response time between “this person is deteriorating” and “this person is receiving intervention” is minutes, not hours.
Outpatient programs operate on a different model. Monitoring is scheduled. Between visits, patients self-report symptoms, follow medication protocols at home, and contact the clinic if something feels wrong. The system works when withdrawal follows a predictable, low-risk trajectory. It gets precarious when something unexpected develops overnight — a seizure with no one present, a rapid escalation in symptoms that doesn’t get recognized in time.
SAMHSA’s treatment data consistently supports the idea that level of care should be matched to clinical risk, not preference. The liability of outpatient isn’t that the therapy is weaker — it’s that the emergency response capacity is structurally limited by design.
Why Home Detox Is Different From Outpatient Detox
Outpatient detox and detoxing at home alone are not the same thing. Not even close. Outpatient programs involve physician-prescribed medications, clinical assessment at every visit, lab work, and formal escalation protocols if symptoms worsen. Attempting to stop drinking without any medical oversight — regardless of how “mild” someone believes their dependence to be — carries a genuine risk of undetected seizure or severe withdrawal. This distinction tends to get lost when people research options online, and it’s worth being explicit about.
Cost and Time Tradeoffs
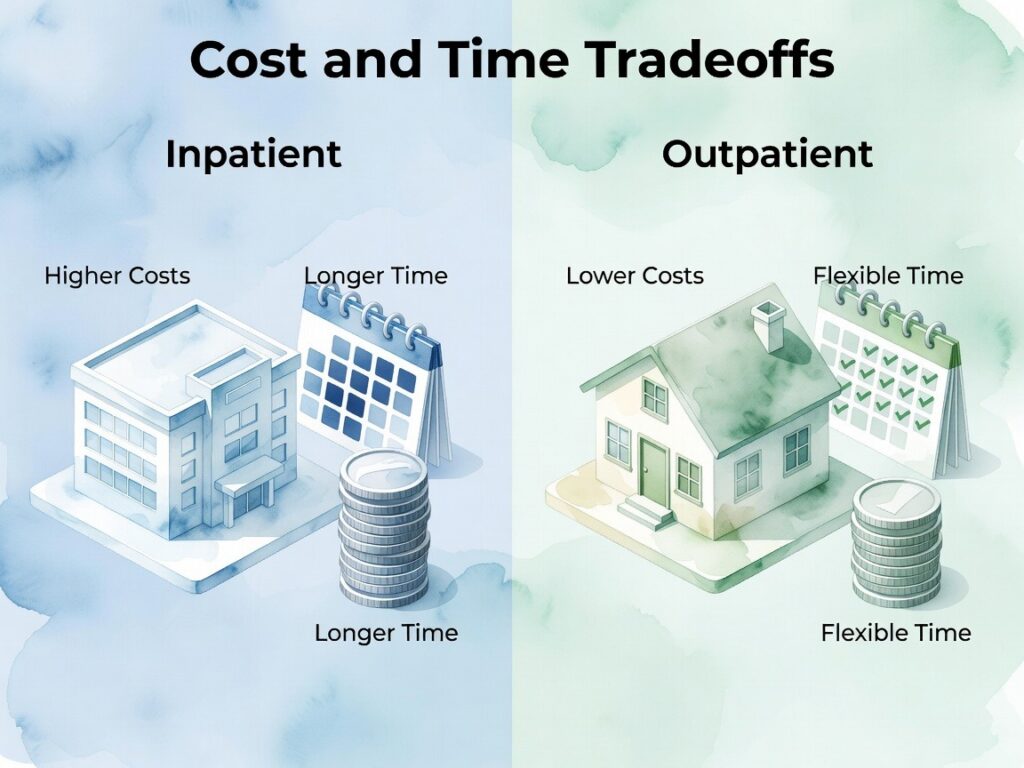
Inpatient detox costs more. That’s simply true. Residential care, depending on the facility, location, and insurance situation, can run anywhere from several hundred to several thousand dollars per day. Outpatient programs cost a fraction of that — sometimes covered more generously by insurance because the ASAM Levels of Care framework classifies them differently. For people without comprehensive coverage, cost is a real and legitimate factor in the decision.
The time commitment differs too. Inpatient requires stepping away from work, childcare, and other obligations for the duration of the stay. That’s hard for a lot of people. Outpatient allows someone to maintain some daily responsibilities, though usually not at full capacity during the detox period. The honest caveat here is that prioritizing work over appropriate medical care during alcohol withdrawal can have consequences far more severe than a week’s absence. Understanding the full picture of what detox involves — including what to expect financially — helps people plan realistically rather than defaulting to whatever sounds least disruptive.
How Clinicians Decide Your Level of Care
No reputable clinician decides your detox setting based on what you prefer or what fits your schedule. The decision is driven by a structured clinical assessment, and it pulls from multiple dimensions simultaneously.
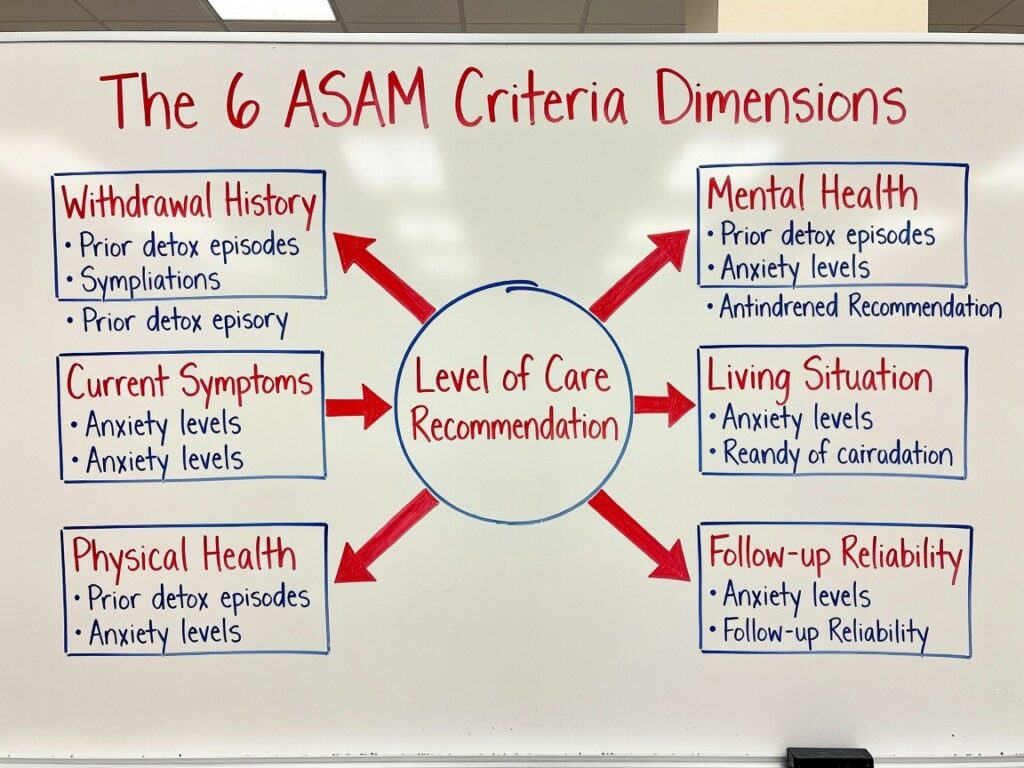
Withdrawal history is weighted heavily because prior complicated withdrawals are among the strongest predictors of future complicated withdrawals. Current symptom severity matters, measured through validated tools. Physical health — liver function, cardiovascular status, nutritional state — shapes what medications are safe to use and how much monitoring is required. Mental health history, particularly co-occurring conditions like severe anxiety, bipolar disorder, or PTSD, adds layers of complexity that can tip a borderline case toward inpatient. And then there’s the social dimension: who’s at home, how stable that environment is, and whether the patient can be trusted to attend follow-up visits.
The ASAM Criteria organizes this into six dimensions that get evaluated simultaneously. It’s not a checklist — it’s a clinical picture. The outcome is a level-of-care recommendation that reflects the intersection of all those factors, not just one or two.
Questions You Can Expect During Assessment
- How much are you drinking daily, and for how long?
- Have you ever had a seizure during a previous withdrawal attempt?
- Do you have any diagnosed medical or psychiatric conditions?
- What medications are you currently taking?
- Who lives with you, and are they supportive of your recovery?
Matching the Setting to Your Life

Work obligations matter. So does childcare. So does transportation. So does whether your apartment has a bottle in the cupboard and a roommate who isn’t sober. These aren’t reasons to choose one setting over another — they’re data points that inform what’s actually feasible within the level of care a clinician recommends.
Is outpatient detox safe depends on the person’s alcohol use history, health, and withdrawal risk. It can be safe for individuals with mild to moderate dependence and stable support systems, where symptoms are expected to be less severe.
However, for heavy drinking or a history of severe withdrawal, outpatient detox may not provide enough medical supervision. In those cases, inpatient care is typically safer due to continuous monitoring and faster response to complications.
The safest option should always be based on a clinical assessment, not convenience.
A 2019 NIH review on outpatient detoxification put it plainly: appropriately selected patients in outpatient settings do as well as inpatient counterparts. The emphasis on “appropriately selected” is doing a lot of work in that sentence. The selection is clinical, not personal.
Not Sure Which Option Fits You?
Most people don’t know which setting they need before they talk to someone. That’s normal — it’s not a decision that can be made reliably from a website, including this one. A formal detox assessment takes 45 minutes to an hour, covers the clinical dimensions that actually predict withdrawal risk, and gives a clinician enough information to make a genuinely individualized recommendation.
Outpatient alcohol detox allows individuals to receive medical assessment, monitoring, and withdrawal support without staying overnight in a facility. Instead of 24/7 supervision, patients attend scheduled appointments where clinicians evaluate symptoms, adjust medications if needed, and track progress throughout the withdrawal period.
Kora Behavioral Health alcohol detox offers alcohol detox services in Lancaster and throughout Central Pennsylvania, including York, Harrisburg, Hershey, Reading, and Lebanon. If you’re trying to decide whether inpatient or outpatient detox is the right fit, the most important next step is speaking directly with a clinician who can assess your situation rather than relying on general guidance alone.
Talk to a clinician about which detox level fits your situation. Free assessment available. Call (866) 861-9667.
FAQs
Is outpatient alcohol detox safe?
Outpatient alcohol detox can be safe for carefully selected individuals — specifically, those with mild-to-moderate withdrawal risk, stable housing, and a reliable support system. It requires consistent medical oversight and isn’t appropriate for everyone. A predictors study published on PubMed identifies the factors most associated with successful outpatient detox outcomes, and clinical evaluation determines whether a given person meets those criteria. Without an assessment, there’s no safe way to know.
How do I know if I need inpatient detox?
A medical assessment is the only reliable way to determine this. That said, prior alcohol-related seizures, a history of delirium tremens, heavy long-term drinking, or significant co-occurring medical conditions all substantially increase the likelihood that inpatient monitoring is the safer choice. Safety should come before convenience in that evaluation — alcohol withdrawal can escalate faster and more severely than people expect.
Can I detox while still going to work?
It depends on withdrawal severity and what the treating clinician recommends. Some outpatient candidates with mild risk profiles may be able to maintain limited daily activities during detox. Many people, even those in outpatient programs, need to reduce or pause work obligations during the active detox period. Following medical guidance rather than work demands is the right frame here — a week away from work is recoverable; an unmanaged withdrawal seizure is not.

